

Category Health & Wellbeing
A vision of health and wellbeing that focuses on quality of life and promoting wellbeing for all across the life course
AllArts, Culture & CreativityClimate, Environment & SustainabilityDemocracy, Justice & GovernanceFuture of WorkHealth & WellbeingResilient, Inclusive CommunitiesTransformative Technology

Detoxifying masculinity: How men’s groups reshape attitudes

Striving for transparency: Why Canada’s pesticide regulations need an overhaul

Detangling the roots and health risks of hair relaxers – Listen, with Cheryl Thompson
Counting carbs with AI for real-time glucose monitoring

Smart wearables that measure sweat provide continuous glucose monitoring

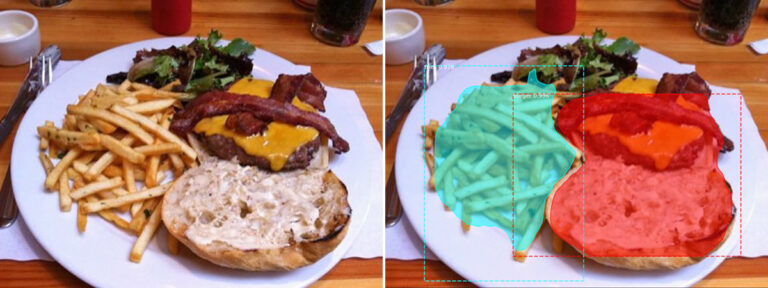
Food for thought: How your mindset can make healthy food more alluring on social media

Lowering carbon emissions by optimizing energy retrofits

An emergency in the making: Ending pandemic prenatal health coverage for uninsured people is both costly and dangerous

Freshwater ecosystems are becoming increasingly salty. Here’s why this is a concern

Rooms with a view: Opening doors to new health care approaches
